
The Neurofeedback Map: Reading Your Teen’s Brain Training Results
Your teen just completed their first QEEG neurofeedback assessment, and now you’re holding a report filled with color-coded brain maps, frequency charts, and terminology that reads like it was written for a graduate neuroscience seminar. You’re not alone in feeling lost. Most parents who walk into my Edmond, OK counseling office for the first time feel exactly that way — curious, hopeful, and a little overwhelmed by the data in front of them.
The neurofeedback map is one of the most valuable tools I use to guide brain training for teens. It replaces guesswork with objective data, giving us a real picture of how your teenager’s brain is functioning — not just a list of symptoms. This article walks you through what a QEEG neurofeedback map shows, how I use that data to build a personalized training plan, and what you can expect as your teen’s brain training progresses. By the time you finish reading, the report in your hands will make a lot more sense.
What a QEEG Neurofeedback Map Actually Shows
A QEEG — Quantitative Electroencephalogram — records electrical activity across the surface of your teen’s brain and then translates that data into a visual map. The “quantitative” part matters: unlike a standard EEG used in hospitals to detect seizures, a QEEG measures brainwave patterns and compares them statistically against a large normative database. I use Jewel QEEG reports in my practice, which cross-reference findings against the QEEG-PRO database — one of the most rigorously maintained normative databases available. That comparison is what separates a real brain map from a glorified relaxation reading.
The map displays activity in four primary brainwave frequencies: delta (0.5–4 Hz), theta (4–8 Hz), alpha (8–12 Hz), and beta (12–30 Hz), along with high beta above 30 Hz. Each frequency band reflects a different type of brain state. Delta dominates during deep sleep. Theta shows up during drowsy, inward, or creative states. Alpha reflects calm, idle alertness — the mental state between focused and resting. Beta supports active thinking, concentration, and problem-solving. High beta is often associated with anxiety, hypervigilance, or cortical overactivation.
The color coding in a QEEG report is not random. Areas shown in warmer colors like red and orange indicate that a particular frequency is running significantly above the norm for your teen’s age group. Cooler colors — blues and greens — point to areas of underactivation. A large swath of elevated theta in the frontal lobe correlates strongly with attention difficulties and the kind of mental fog that makes sustained focus feel impossible. Elevated high-beta in the temporal regions often tracks with anxiety or a nervous system stuck in a stress response.
What the map does not do is diagnose a condition by itself. I treat it as one critical layer of data alongside a thorough intake conversation, behavioral observations, and your own knowledge of your teen as a parent. The map tells me what the brain is doing; you help me understand what that looks like in your teenager’s daily life — at school, at home, on the field, or in relationships.
Why Normative Database Comparison Matters
The QEEG-PRO database that anchors Jewel QEEG reports contains brainwave data from thousands of neurologically typical individuals across different age groups. When your teen’s recording gets analyzed, it isn’t compared to a generic adult standard — it’s compared to age-matched peers. This matters for parents of teenagers because adolescent brain development is genuinely different from adult brain patterns. Theta-to-beta ratios shift substantially during the teen years, and a provider who doesn’t account for those developmental norms risks misreading the map entirely.
This is also why I chose to invest in BCIA certification — the credential issued by the Biofeedback Certification International Alliance. BCIA-certified providers complete a rigorous education and training sequence that includes neuroanatomy, supervised clinical hours, and a comprehensive certification exam. BCIA is recognized by the three major international organizations in neurofeedback and biofeedback, and the certification exists to ensure that practitioners who work with QEEG data and brain training protocols actually know what they’re looking at. Not every provider offering neurofeedback holds this credential. I do, and it shapes how I read every map I review.
What the Intake Process Looks Like Before We Map Anything
Before your teen ever sits down for a QEEG recording, we spend significant time in conversation. The intake process at my practice is thorough on purpose. A brain map without clinical context is a collection of data points. Clinical context without objective brain data is an educated guess. We need both.
During intake, I gather a detailed picture of your teen’s history — academic performance patterns, behavioral observations at home and school, sleep quality, emotional regulation, social relationships, any prior diagnoses or evaluations, and how they describe their own experience. Parents often notice things about their teenager that the teen can’t or won’t articulate themselves, and that perspective matters.
I also spend time with your teen directly. Adolescents respond differently when they feel like a participant in the process rather than a subject being studied. I explain what the QEEG recording involves — sensors placed on the scalp to measure electrical activity, a non-invasive process that doesn’t hurt or send anything into the brain — and I answer their questions honestly. A teenager who understands what we’re doing and why tends to produce cleaner recordings and engages more meaningfully in the training that follows.
How the Recording Session Works
The QEEG recording itself involves placing a sensor cap on your teen’s head. The sensors pick up the brain’s electrical signals — they don’t transmit, stimulate, or alter anything. Your teen sits comfortably, usually with their eyes open for part of the recording and eyes closed for another segment. The process typically takes around 25 minutes. Many teens find it interesting rather than stressful once they understand that the equipment is simply listening to what their brain is already doing.
After the recording, the raw data gets processed through the Jewel QEEG software and cross-referenced against the QEEG-PRO normative database. The resulting report maps cortical activity across 19 or more electrode sites, giving us a detailed picture of the brain’s functional patterns rather than a single average number.
In-Person and Online Options
We can do your brain map in-person in my Edmond office, however if you can’t come to the office in-person, we can start training online. I have trained people hundreds of miles away, who may come by my office when they are swinging through town. Online training is done on an iPad, which makes the setup straightforward for families who aren’t geographically close. The brain map itself does require that initial in-person visit — it’s the foundation everything else is built on — but once we have that data in hand, ongoing training sessions can happen remotely, self-paced, with my oversight throughout.
Reading the Map: What Each Frequency Pattern Can Suggest
No two QEEG reports look identical, and that’s the whole point. I want to walk you through the most common patterns I see in teens, along with what those patterns tend to correlate with clinically. These are tendencies, not diagnoses. The goal is to give you a framework so that when we review your teen’s map together, you’re oriented rather than adrift.
Elevated Frontal Theta — The Focus Problem
One of the most frequent patterns in teens referred for attention difficulties is an excess of slow theta waves in the frontal and central regions of the brain. Research consistently links elevated theta and reduced beta activity in the frontal regions to inattention and impaired cognitive control, the kind of pattern associated with ADHD-like symptoms. For a teenager, this can show up as chronic difficulty starting tasks, losing track mid-assignment, mental fogginess that doesn’t lift with sleep, and a persistent sense that their brain just won’t cooperate.
Neurofeedback training targeting this pattern works by rewarding the brain when it produces more beta activity in those specific regions and less theta. Over many sessions, the brain learns to regulate itself more efficiently. The key word is “learns” — this is operant conditioning applied to brainwave patterns, not a temporary chemical effect that reverses when a pill wears off.
ADHD and the Busier Brain Presentation
I’ve seen a couple of presentations of ADHD in my office, and many times it’s a busier brain presentation, which looks like an anxious brain. This is worth naming clearly because it changes the clinical picture considerably. When a parent describes their teen as scattered, impulsive, and wound up — and the brain map confirms elevated high-beta alongside the theta excess — the standard “calm down and focus” framing doesn’t fully apply. The brain isn’t just under-activated in its attention networks; it’s also running hot in ways that make the whole system harder to regulate. Training protocols for this pattern look different from a simple theta-suppression approach, and misreading it leads to protocols that help in one direction while worsening another.
Elevated High Beta — The Anxiety Signature
High-beta excess, particularly in the frontal and temporal regions, shows up frequently in teens struggling with anxiety, chronic worry, and hypervigilance. A brain running too much high-beta is stuck in an elevated threat-detection state. These are the teenagers who can’t quiet racing thoughts at night, who catastrophize before tests, who feel chronically tense even in objectively safe situations.
This pattern is one reason I find the objective map so clinically useful. Anxiety in teenagers often presents as irritability, avoidance, or what parents describe as “drama.” Without a map, the presentation can be misread as behavioral. The QEEG shows that the nervous system is genuinely overactivated — which changes how we approach treatment and also how parents can understand what their teen is experiencing.
Alpha Suppression — The Transition Problem
Alpha waves normally serve an idling function. When the brain shifts between tasks or winds down after stimulation, alpha helps that transition happen smoothly. Teens with insufficient alpha often struggle with transitions — between activities, between emotional states, between periods of high demand and rest. They tend to stay activated when they should be de-escalating, which feeds both sleep problems and emotional volatility.
Coherence and Connectivity Patterns
Beyond raw brainwave frequencies, the Jewel QEEG report examines coherence — how well different regions of the brain communicate with each other. Abnormal coherence patterns can suggest underconnected or overconnected brain networks. Underconnectivity between the frontal and parietal lobes often correlates with executive function difficulties. Overcoherence in certain networks can indicate rigidity in thinking or processing. This layer of the map is one that many providers skip, relying only on the basic power analysis. I don’t, because connectivity patterns often explain symptoms that the power maps alone leave unaccounted for.
How the Map Becomes a Personalized Brain Training Protocol
After reviewing your teen’s QEEG data, I don’t pull a pre-set program off a shelf. The map tells me which electrode sites need attention, which frequency bands we’re targeting, whether we’re working to increase or decrease a particular type of activity, and in what sequence. Two teenagers who both carry an ADHD diagnosis can have meaningfully different brain maps — and they should have meaningfully different training protocols as a result.
This is where my BCIA certification directly affects your teen’s care. Reading a QEEG report accurately and translating it into an appropriate neurofeedback protocol requires training that goes well beyond purchasing equipment and learning to operate software. The BCIA certification pathway requires supervised clinical hours, case presentations, and demonstrated competency with a range of presentations. It’s the difference between a provider who uses neurofeedback as an add-on service and one who has trained specifically in the neuroscience behind it.
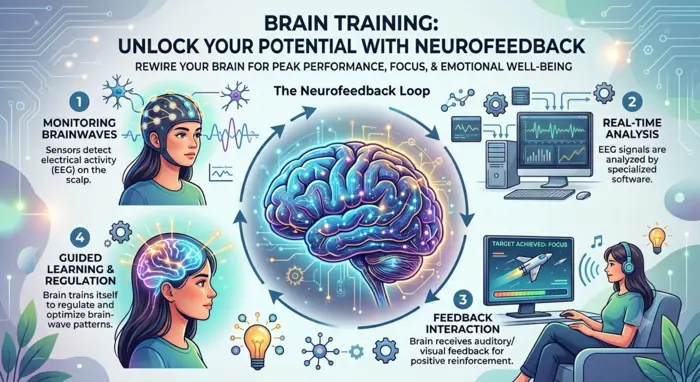
Sessions typically run around 25 minutes. Your teen sits comfortably while sensors relay real-time brainwave data to software that provides feedback — usually visual or auditory — whenever their brain hits the target pattern we’ve set. The brain responds to that feedback by learning to produce more of the desired state. This happens below the level of conscious effort, which is why teens who are skeptical about “mind training” often find themselves reporting changes they didn’t expect.

What Progress Monitoring Looks Like After Training Begins
Neurofeedback is not a treatment you set in motion and forget. I monitor results throughout the process, and what we see in the data informs whether we stay the course, adjust the protocol, or shift focus to a different brain region. This ongoing clinical oversight is one of the things that separates brain map-guided neurofeedback from consumer EEG devices that let users train on their own at home.
Parent observations matter here. You live with your teenager. You notice changes I can’t see in a 25-minute session — shifts in sleep quality, emotional volatility, focus at homework time, how they handle a frustrating situation compared to six weeks ago. I ask for that feedback systematically, because the map tells me about brain states and your reports tell me about real-world function. Both streams of information guide how I manage the protocol.
When to Expect Changes — and How They Happen
Most families start noticing something within 10 to 20 sessions, though the nature of those changes varies by teen and by what we’re training. Sleep often improves early in the process. Focus and emotional regulation changes tend to show up next, followed by more stable mood patterns over time. Some changes are gradual enough that parents don’t notice them until they realize it’s been two weeks since the last meltdown, or their teen mentioned that school feels less overwhelming.
Neurofeedback changes are learned, not imposed. The brain is building new patterns of self-regulation through repeated practice. This is why the research on neurofeedback outcomes tends to show durability — the brain retains what it learns. That said, the number of sessions needed, the pace of progress, and the specific outcomes depend on your teen’s individual profile. I don’t make uniform promises about results because no two brains follow the same path.
Why Objective Brain Data Changes the Conversation
Most mental health treatment — even good, evidence-based treatment — relies heavily on subjective reporting. A teen describes what they feel, a clinician observes behavior, a checklist gets scored. These tools have real value. But they also depend on the teen’s ability and willingness to communicate accurately, and they miss what’s happening underneath the behavioral surface.
The neurofeedback map gives us objective data that exists independent of how well your teenager can articulate their experience. For many adolescent boys in particular, the question “how are you feeling?” hits a wall. The brain map doesn’t ask. It shows. That shift — from subjective report to objective measurement — often changes how teens relate to their own treatment. When a 15-year-old can see his own theta excess on a brain map, the explanation for why focus has always been a battle becomes concrete rather than abstract. That clarity tends to motivate engagement in ways that abstract reassurance rarely does.
It also gives me a more precise target. Rather than applying a general CBT or ACT framework to a vague presentation, I can combine those approaches with a brain training protocol that addresses the specific neurological pattern driving the struggle. The therapeutic modalities I use in my counseling work and the neurofeedback training reinforce each other in ways that neither achieves independently.
What to Look for in a Neurofeedback Provider for Your Teen
Parents doing their research will quickly discover that neurofeedback is offered by a wide range of providers — from licensed therapists to wellness centers and unlicensed practitioners. The quality of care within that range varies considerably. Here are the questions worth asking before you commit.
First: Is the provider BCIA certified? BCIA certification is the field’s primary independent credential. The certification requires demonstrated competency in neurofeedback practice, supervised clinical training, and ongoing continuing education. It signals that the provider has gone beyond simply purchasing equipment.
Second: Do they use a normative database for QEEG analysis? Brain training without a normative reference point leaves the provider flying on intuition rather than data. Jewel QEEG reports with QEEG-PRO database comparison give my practice a scientific anchor that generic systems don’t provide.
Third: Is the intake process thorough? A QEEG assessment done in isolation from a clinical interview produces an incomplete picture. The map should inform a treatment relationship, not replace one.
Fourth: Do they monitor and adjust? Neurofeedback protocols that never change regardless of how the teen responds are not being managed — they’re just being administered. Clinical oversight means the provider is actively tracking both brain data and behavioral outcomes throughout the training process.
Quick Takeaways
- A QEEG neurofeedback map measures your teen’s brainwave activity and compares it against an age-matched normative database — it shows what the brain is actually doing, not just what the teen reports feeling.
- Jewel QEEG reports cross-referenced with the QEEG-PRO database provide one of the most rigorous normative comparison frameworks available, anchoring every protocol I build.
- Different frequency patterns — elevated theta, high-beta excess, alpha suppression, coherence abnormalities — correlate with specific challenges like attention difficulties, anxiety, and emotional dysregulation.
- ADHD doesn’t always look like a sluggish brain. Many times it presents as a busier, more anxious-looking brain — and the treatment protocol needs to reflect that distinction.
- BCIA certification means the provider has met a nationally recognized standard of training — an important credential to verify before starting any neurofeedback program.
- Brain training can be done in-person in Edmond or remotely on an iPad, with progress monitored throughout regardless of where your teen trains.
- The map becomes the foundation of a personalized training protocol. No two teens receive the same plan, even when their presenting symptoms look similar.
Ready to Look at What’s Actually Happening in Your Teen’s Brain?
If your teenager has been struggling — with focus, anxiety, emotional regulation, sleep, or some combination of all of these — and the approaches you’ve tried so far have produced limited results, the neurofeedback map is worth understanding. Not because it’s a cure, but because it asks a different question. Instead of asking what symptom your teen has, it asks what the brain is doing to produce that symptom. That shift in frame opens up a more precise and more durable path to change.
In my Edmond, OK practice, I work with teens and their families through a thorough intake process that combines clinical conversation with objective QEEG data. Every brain training protocol I develop is built from that individual map — not from a diagnostic category or a generic program. I hold BCIA certification because this field requires real training to practice responsibly, and I take that seriously.
If you’re ready to explore what QEEG-guided neurofeedback might look like for your teenager, reach out and schedule a consultation. The first conversation is straightforward — we talk about your teen, answer your questions, and figure out whether this is the right fit.
Have questions about neurofeedback for your teen? I work with families in Edmond and across the country.
Schedule a consultation today — or learn more about how I use QEEG brain maps in my practice.
Frequently Asked Questions About Neurofeedback Maps and Teen Brain Training
The recording itself runs around 25 minutes. The full intake appointment, which includes the QEEG plus the clinical interview, typically takes two to three hours. To prepare, your teen should arrive well-rested if possible, avoid caffeine on the day of the assessment, and come with clean, dry hair — conditioners and heavy styling products can interfere with sensor contact. I walk every family through the preparation checklist ahead of their appointment so nothing gets missed.
Yes. The QEEG recording is entirely non-invasive — the sensors read electrical activity but send nothing into the brain. The neurofeedback training itself involves operant conditioning of brainwave patterns through audio or visual feedback. It doesn’t use medication, electrical stimulation, or physical intervention of any kind. Some teens experience mild fatigue after early sessions as their brain adjusts to the training demands. This is normal and typically resolves within a few sessions.
My practice does not bill insurance for neurofeedback services. This is a private-pay service, and the investment varies based on the scope of care your teen’s protocol requires. I encourage families to contact me directly to discuss specifics. Many families find that the ability to access individualized, clinically supervised brain training without insurance restrictions is worth the trade-off.
There’s no single answer to this, which I recognize is frustrating when you’re trying to plan. The number of sessions depends on your teen’s specific brain map, the nature and severity of the challenges we’re addressing, and how the brain responds to training. Most protocols run in the range of 20 to 40 sessions, with periodic progress reviews built in. I don’t lock families into a fixed package upfront — I monitor results and we make decisions about the arc of care together as training progresses.
A traditional psychological evaluation relies primarily on standardized tests, clinical interviews, behavior rating scales, and self-report. These are valuable tools, but they measure function indirectly through behavior and self-perception. The QEEG neurofeedback map measures the brain’s electrical activity directly and compares it against a normative database of age-matched peers. The two approaches address different questions and are often complementary. I use the QEEG map alongside — not instead of — a thorough clinical intake process.
Your Turn
If your teen has already had a QEEG assessment, what was the part of the report you found hardest to understand? Drop a question in the comments or send me a message directly — I’m happy to help demystify the data. And if this article was helpful, consider sharing it with another parent who’s navigating the same territory. Brain training for teens is still a field that many families haven’t heard of, and straightforward information is hard to come by.
References
- Kopańska, M., & Trojniak, J. (2025). From aberrant brainwaves to altered plasticity: A review of QEEG biomarkers and neurofeedback in the neurobiological landscape of ADHD. Cells, 14(17). ncbi.nlm.nih.gov
- Biofeedback Certification International Alliance (BCIA). Board certification in neurofeedback. bcia.org
- Bitbrain. (2025). What is QEEG brain mapping and how to interpret it. bitbrain.com
- NIH/NCBI. (2025). Neurofeedback for ADHD: Exploring the role of quantitative EEG and brainwave modulation. ncbi.nlm.nih.gov
- School of Neurotherapy. BCIA board certification for neurofeedback. schoolofneurotherapy.com